Related Concept Videos
 01:27
01:27Oxygen Transport in the Blood
 01:21
01:21Acute Respiratory Failure-II
The underlying physiological abnormalities that contribute to hypoxemic respiratory failure include:
 01:23
01:23Acute Respiratory Failure-IV
 01:24
01:24Muscle Recovery and Fatigue
 01:19
01:19Special considerations while measuring oxygen saturation
Ensuring accuracy in vital sign recordings while prioritizing patient comfort and minimizing anxiety is important.
 01:30
01:30Acute Respiratory Failure-III
You might also read
Related Articles
Articles linked to this work by shared authors, journal, and citation graph.
Effect of acute hypoxia on central fatigue during repeated isometric leg contractions.
Evidence of decrease in peak heart rate in acute hypoxia: effect of exercise-induced arterial hypoxemia.
A high blood lactate induced by heavy exercise does not affect the increase in submaximal VO2 with hyperoxia.
Related Experiment Video
Updated: Jul 13, 2026
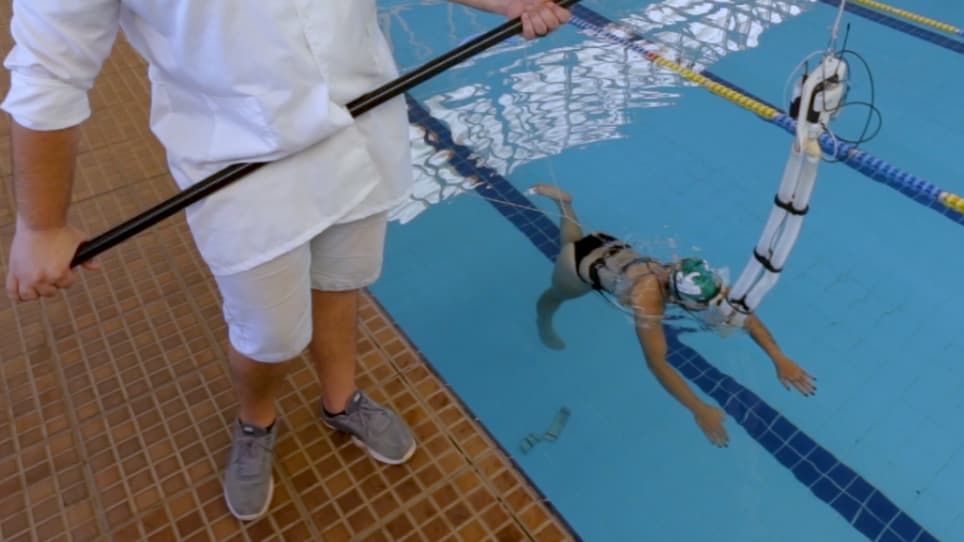
A Rapidly Incremented Tethered-Swimming Maximal Protocol for Cardiorespiratory Assessment of Swimmers
Published on: January 28, 2020
Accumulated oxygen deficit during ramp exercise.
1Unité de Recherche Physiologie et Physiopathologie de l'Exercice et Handicap, Université de St-Etienne, France. JP.Pouilly@univ-st-etienne.fr
Maximal oxygen deficit (MAOD) during ramp exercise is comparable to oxygen deficit during constant-power tests. However, oxygen lag during ramp exercise is not a reliable indicator due to high variability.
More Related Videos
 08:44
08:44Dual Test Gas Pulmonary Diffusing Capacity Measurement During Exercise in Humans Using the Single-Breath Method
Published on: February 2, 2024
 07:09
07:09Assessment of Pulmonary Capillary Blood Volume, Membrane Diffusing Capacity, and Intrapulmonary Arteriovenous Anastomoses During Exercise
Published on: February 20, 2017
Area of Science:
- Exercise Physiology
- Sports Science
Background:
- The oxygen deficit represents the difference between oxygen required and oxygen actually consumed during exercise.
- Accurate measurement of oxygen deficit is crucial for understanding exercise physiology and performance.
Purpose of the Study:
- To compare oxygen deficit during ramp exercise (OD ramp and OD lag) with maximal oxygen deficit (MAOD) from a constant-power test.
- To assess the reliability of different oxygen deficit measurements during incremental exercise.
Main Methods:
- 12 healthy males performed ramp exercise tests at 15 W.min(-1) and 30 W.min(-1) to determine OD ramp and OD lag.
- Maximal oxygen deficit (MAOD) was determined from an exhaustive constant-power test at 105% of peak power output.
- OD ramp and OD lag were calculated using established methods comparing oxygen demand with oxygen uptake.
Main Results:
- OD ramp from both 15 W.min(-1) and 30 W.min(-1) ramp tests did not significantly differ from MAOD.
- OD lag from 15 W.min(-1) ramp tests was not significantly different from MAOD.
- OD lag from 30 W.min(-1) ramp tests was significantly greater than MAOD (p < 0.05).
- Test-retest variability was elevated for OD lag measurements.
Conclusions:
- Oxygen deficit accumulates progressively during ramp exercise, potentially reaching MAOD.
- OD ramp appears to be a valid measure comparable to MAOD.
- OD lag, particularly at higher ramp rates, may overestimate the true oxygen deficit and shows high variability, limiting its reliability as an individual index.