Related Concept Videos
 01:26
01:26Urinary Tract Calculi II: Pathophysiology and Clinical Manifestations
Renal calculi, commonly termed kidney stones, are crystalline solid masses that form in the kidneys but can occur at any point within the urinary system, encompassing the kidneys, ureters, bladder, and urethra.The pathophysiology of renal stones involves several key factors: supersaturation of the urine with stone-forming constituents, changes in urine pH, a decrease in urine volume, and the presence of substances that promote or inhibit stone formation.Supersaturation of Urine: This is the...
 00:51
00:51Synthesis and Functions of Calcitonin
Calcitonin, a vital polypeptide hormone, regulates calcium levels within body fluids. It is released by the parafollicular cells, also known as C cells, situated in the follicular epithelium of the thyroid gland. Calcitonin responds to fluctuations in blood calcium levels and the influence of gastrointestinal hormones like gastrin and cholecystokinin.
The exact mechanisms by which calcitonin operates in calcium homeostasis remain elusive, but its significance is evident in several vital...
The exact mechanisms by which calcitonin operates in calcium homeostasis remain elusive, but its significance is evident in several vital...
 01:28
01:28Urinary Tract Calculi I: Introduction
Renal calculi, or kidney stones, are solid deposits of minerals and salts formed inside the kidneys. In medical terminology, "calculus" refers to the stone itself, while "lithiasis" describes the process of stone formation. Depending on their location within the urinary system, these stones may be classified as either urolithiasis, when situated within the urinary tract, or nephrolithiasis, when located within the kidneys. Each term signifies the specific impact of the stone.Predisposition...
 01:21
01:21Skeleton and Calcium Homeostasis
Calcium is not only the most abundant mineral in bone but also the most abundant mineral in the human body. Calcium ions are needed for bone mineralization, tooth health, heart rate regulation and strength of contraction, blood coagulation, the contraction of smooth and skeletal muscle cells, and the regulation of nerve impulse conduction. The average calcium level in the blood is about 10 mg/dL. When the body cannot maintain this level, a person will experience hypo or hypercalcemia.
 01:28
01:28Antihypertensive Drugs: Potassium-Sparing Diuretics
Liddle syndrome is a genetically inherited form of hypertension characterized by the overactivity of epithelial sodium channels in the nephron, the functional unit of the kidney. This heightened activity leads to increased sodium reabsorption and excessive excretion of potassium. To counteract this, potassium-sparing diuretics such as amiloride are used. They function by blocking these sodium channels, thereby reducing the influx of sodium into the epithelial cells and minimizing the loss of...
 01:21
01:21Huntington Disease l: Introduction
Huntington disease or HD is a progressive, fatal neurodegenerative disorder inherited in an autosomal dominant pattern.PathophysiologyIt is caused by expansion of the CAG trinucleotide repeat in the HTT gene on chromosome 4 (4p16.3), producing an abnormal huntingtin protein with an expanded polyglutamine tract. This misfolded protein disrupts cellular function, leading to neuronal death. Normal alleles have ≤26 repeats, 27–35 are intermediate (risk of expansion), 36–39 show reduced penetrance,...
You might also read
Related Articles
Articles linked to this work by shared authors, journal, and citation graph.
Sort by
Same author
Multiple endocrine neoplasia type 2: From molecular genetics to precision therapy.
Best practice & research. Clinical endocrinology & metabolism·2026
Same author
Safety of biopsy in phaeochromocytoma and paraganglioma: an international, multicentre, retrospective cohort study.
The lancet. Diabetes & endocrinology·2026
Same author
Approach to the Patient with Metastatic Pheochromocytoma and Paraganglioma: Advances in Systemic Therapy.
The Journal of clinical endocrinology and metabolism·2026
Related Experiment Video
Updated: Jun 2, 2026
07:13
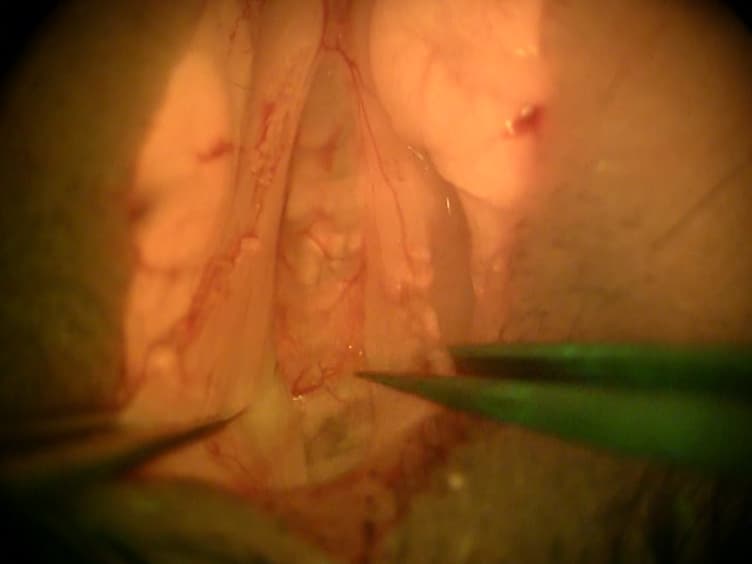
Two Techniques to Create Hypoparathyroid Mice: Parathyroidectomy Using GFP Glands and Diphtheria-Toxin-Mediated Parathyroid Ablation
Published on: March 14, 2017
Benign familial hypocalciuric hypercalcemia.
Jeena Varghese1, Thereasa Rich, Camilo Jimenez
1Department of Endocrine Neoplasia and Hormonal Disorders, The University of Texas MD Anderson Cancer Center, Houston, Texas 77030, USA.
Summary
Benign familial hypocalciuric hypercalcemia, caused by CASR gene mutations, presents lifelong hypercalcemia. Early diagnosis is crucial to avoid unnecessary parathyroidectomy and manage this benign condition effectively.

Area of Science:
- Endocrinology
- Genetics
- Calcium Metabolism
Background:
- Benign familial hypocalciuric hypercalcemia (BFHH) is a genetic disorder causing lifelong hypercalcemia.
- It is often mistaken for primary hyperparathyroidism, leading to potential misdiagnosis and inappropriate treatment.
- The condition stems from mutations in the calcium-sensing receptor gene (CASR).
Purpose of the Study:
- To review the pathophysiology, clinical features, diagnosis, and management of BFHH.
- To differentiate BFHH from primary hyperparathyroidism.
- To emphasize the importance of avoiding surgical intervention in BFHH patients.
Main Methods:
- Systematic literature review of available studies on BFHH.
- Analysis of genetic causes, clinical presentation, and diagnostic criteria.
- Evaluation of management strategies and patient outcomes.
Main Results:
- BFHH is an autosomal dominant condition with lifelong hypercalcemia, relative hypocalciuria, and elevated parathyroid hormone.
- CASR gene loss-of-function mutations are the underlying cause.
- Complications like osteopenia and nephrolithiasis are not increased in BFHH, and parathyroidectomy is not recommended.
Conclusions:
- BFHH is an important, though uncommon, cause of hypercalcemia, particularly in younger individuals.
- Diagnosis is critical to prevent unnecessary parathyroidectomy, as hypercalcemia persists post-surgery.
- Genetic screening and family member evaluation are essential for proper management and patient counseling.