Related Concept Videos
 01:22
01:22Trachea
The trachea, commonly known as the windpipe, is a vital part of the human respiratory system. It serves as a passageway for air to travel between the larynx and the bronchi, allowing oxygen to reach the lungs. Let's explore its anatomical features, dimensions, layers of the tracheal wall, associated muscles, and the functions of its parts.
Anatomical Features:
Location: About half of the trachea is situated in the neck, anterior to the esophagus, and extends from the larynx (at the level of the...
Anatomical Features:
Location: About half of the trachea is situated in the neck, anterior to the esophagus, and extends from the larynx (at the level of the...
 01:23
01:23Chronic Pharyngitis
Chronic pharyngitis refers to persistent inflammation of the pharyngial mucosa.
Etiology
It often arises from persistent viral or bacterial infections affecting sinuses and tonsils.
Additional contributing factors include inadequate dental hygiene, mouth breathing, recurring tonsillitis, allergic rhinitis, laryngopharyngeal reflux, and exposure to smoke, chemicals, and other environmental pollutants. Allergic reactions to pollen, mold, and pet dander, chronic cough, excessive voice usage,...
Etiology
It often arises from persistent viral or bacterial infections affecting sinuses and tonsils.
Additional contributing factors include inadequate dental hygiene, mouth breathing, recurring tonsillitis, allergic rhinitis, laryngopharyngeal reflux, and exposure to smoke, chemicals, and other environmental pollutants. Allergic reactions to pollen, mold, and pet dander, chronic cough, excessive voice usage,...
 01:21
01:21Tooth Anatomy
The human tooth enables us to eat a variety of foods, speak clearly, and even aid in shaping our faces. Teeth are composed of various elements that work together. Here's a detailed look at the anatomy of a human tooth.
The Crown, Neck, and Root
The visible part of the tooth is referred to as the crown. It's covered by enamel, the hardest substance in the human body. The crown is uniquely shaped for each type of tooth, allowing for different functions such as cutting, tearing, or grinding food.
The Crown, Neck, and Root
The visible part of the tooth is referred to as the crown. It's covered by enamel, the hardest substance in the human body. The crown is uniquely shaped for each type of tooth, allowing for different functions such as cutting, tearing, or grinding food.
 01:26
01:26Esophageal Strictures-II: Clinical Features and Management
Patients with esophageal strictures often experience a range of symptoms. Initially, they may have difficulty swallowing solid foods, which can progress to include liquids. Additional symptoms may involve chest pain or discomfort, regurgitating food and fluids, heartburn, unintentional weight loss, coughing or choking during meals, and hoarseness.
Healthcare providers should gather a comprehensive medical history and conduct a physical examination for diagnosis. If esophageal stricture is...
Healthcare providers should gather a comprehensive medical history and conduct a physical examination for diagnosis. If esophageal stricture is...
You might also read
Related Articles
Articles linked to this work by shared authors, journal, and citation graph.
Sort by
Same author
Rehabilitation of Maxillectomy Patients Using Zygoma Implants.
Journal of maxillofacial and oral surgery·2025
Same author
Effectiveness of Additive Manufactured Titanium Implants in the Reconstruction of Large Cranial Defects: Case Series and Review of Literature.
Journal of maxillofacial and oral surgery·2024
Same author
The Curious Case of a 'Maverick' Cementoblastoma!
Journal of maxillofacial and oral surgery·2024
Related Experiment Video
Updated: May 29, 2026
06:32
Coronoid-Temporalis Pedicled Flap for Orbital Floor Defect Reconstruction
Published on: December 5, 2025
Coronoid hyperplasia in chronic progressive trismus.
Ashish Chakranarayan1, Priya Jeyaraj
1Oral and Maxillofacial Surgery, Dental Centre, INHS Kalyani, Visakhapatnam 530005, AP, India. ashish_chakranarayan@hotmail.com
Medical Hypotheses
|August 26, 2011
Summary
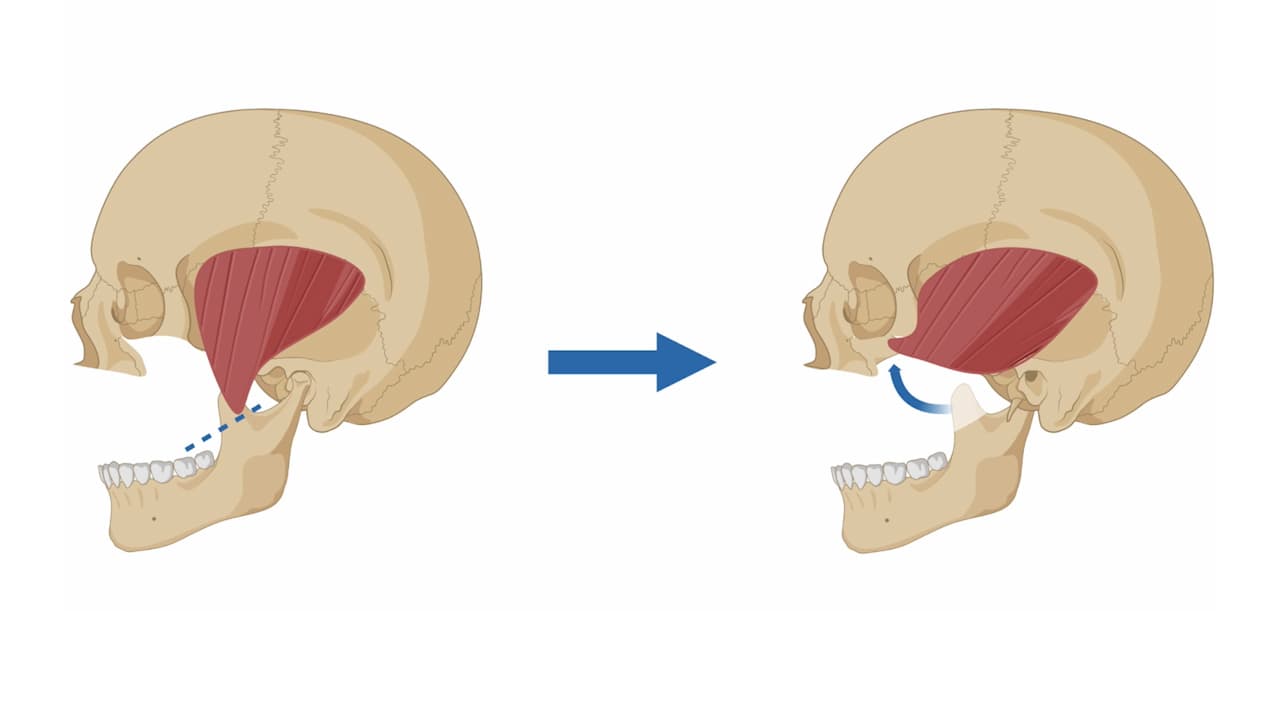
Coronoid hyperplasia, or overgrowth of the mandible's coronoid process, occurs in conditions like oral submucous fibrosis and TMJ ankylosis. This study hypothesizes a common mechanism for this hyperplasia, linked to mandibular hypomobility rather than specific causes.


Area of Science:
- Oral and Maxillofacial Surgery
- Pathology
- Biomedical Engineering
Background:
- Coronoid process hyperplasia is observed in distinct conditions such as oral submucous fibrosis and temporomandibular joint (TMJ) ankylosis.
- The precise etiopathogenesis and mechanisms underlying coronoid overgrowth in these conditions remain inadequately explained.
- Despite etiological differences, progressive hypomobility of the mandible is a common feature in patients with coronoid hyperplasia.
Purpose of the Study:
- To propose a unifying hypothesis for the mechanism of coronoid hyperplasia.
- To explore the role of mandibular hypomobility in the development of coronoid process elongation.
- To elucidate a mechanism for coronoid hyperplasia independent of the primary etiological factors causing trismus.
Main Methods:
- Literature review and analysis of existing case studies on coronoid hyperplasia.
- Comparative analysis of conditions associated with coronoid hyperplasia and mandibular hypomobility.
- Development of a theoretical model hypothesizing the biomechanical factors contributing to coronoid elongation.
Main Results:
- Mandibular hypomobility, irrespective of the underlying cause, appears to be a significant factor in coronoid process hyperplasia.
- A proposed mechanism suggests that altered biomechanical forces due to restricted mandibular movement contribute to coronoid elongation.
- The hypothesized mechanism offers a potential explanation for coronoid hyperplasia in etiologically diverse conditions.
Conclusions:
- Mandibular hypomobility is hypothesized as a common pathway leading to coronoid process hyperplasia.
- The proposed mechanism provides a novel perspective on the etiopathogenesis of coronoid elongation.
- Further research is warranted to validate the proposed biomechanical mechanism of coronoid hyperplasia.