Related Concept Videos
 01:27
01:27Fractures: Bone Repair
Treatment for a fracture is based on the type of break, the bone affected, and the patient's age.
Minor fractures with no bone displacement are treated by immobilizing the fractured bone using a cast or splint. However, in the case of fractures with displaced bones, the broken bones are repositioned before immobilization to ensure successful healing without deformation and loss of function. The realignment of fractured bone ends is performed through a process called reduction. If the procedure...
Minor fractures with no bone displacement are treated by immobilizing the fractured bone using a cast or splint. However, in the case of fractures with displaced bones, the broken bones are repositioned before immobilization to ensure successful healing without deformation and loss of function. The realignment of fractured bone ends is performed through a process called reduction. If the procedure...
 01:27
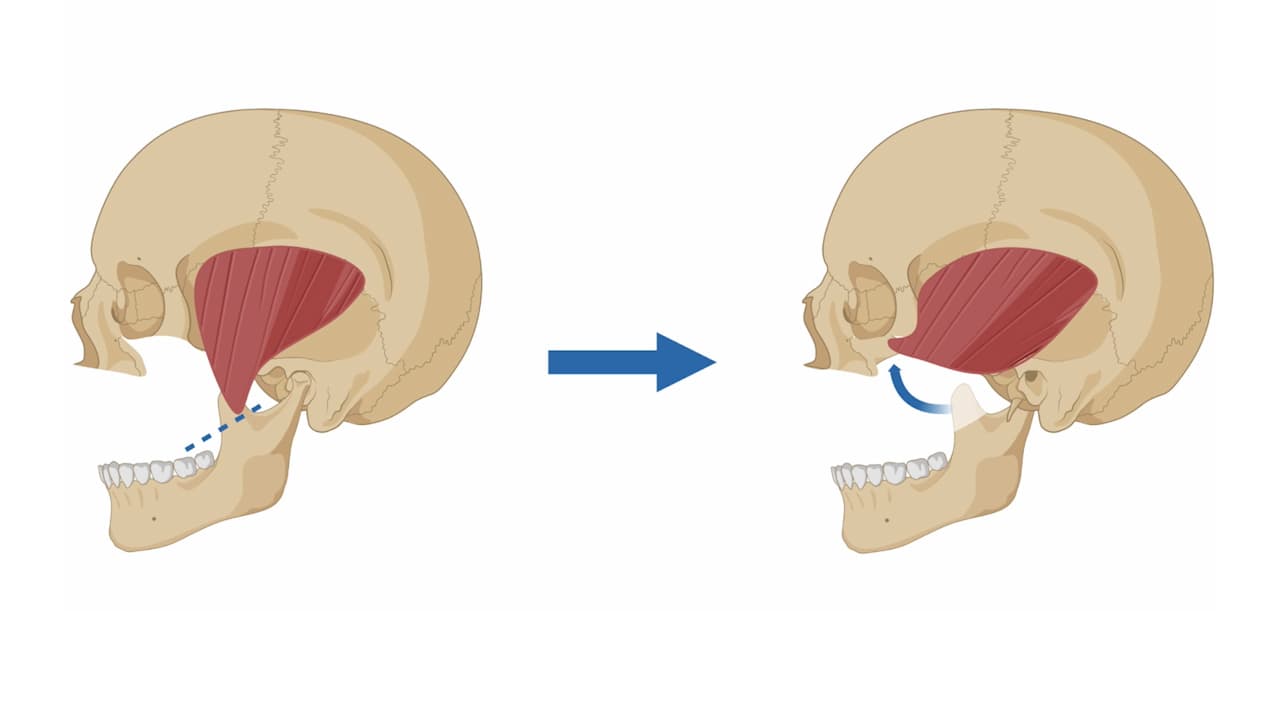
01:27Cranial Bones: Lateral View
The lateral view of the cranium is dominated by temporal, sphenoid, and ethmoid bones.
The temporal bone forms the lower lateral side of the skull. The temporal bone is subdivided into several regions. The flattened upper portion is the squamous portion of the temporal bone. Below this area and projecting anteriorly is the zygomatic process of the temporal bone, which forms the posterior portion of the zygomatic arch. Posteriorly is the mastoid portion of the temporal bone. Projecting...
The temporal bone forms the lower lateral side of the skull. The temporal bone is subdivided into several regions. The flattened upper portion is the squamous portion of the temporal bone. Below this area and projecting anteriorly is the zygomatic process of the temporal bone, which forms the posterior portion of the zygomatic arch. Posteriorly is the mastoid portion of the temporal bone. Projecting...
 01:24
01:24Flail Chest-I
Overview of Flail Chest
Flail chest is a severe and potentially life-threatening condition characterized by the fracture of three or more adjacent ribs in multiple places. It is most commonly caused by direct impacts and trauma, such as motor vehicle accidents or injuries from a steering wheel impact. It can also occur due to falls in elderly individuals with osteoporosis, or assaults involving sharp objects.
Pathophysiology
The pathophysiology of flail chest is complex, involving fractures of...
Flail chest is a severe and potentially life-threatening condition characterized by the fracture of three or more adjacent ribs in multiple places. It is most commonly caused by direct impacts and trauma, such as motor vehicle accidents or injuries from a steering wheel impact. It can also occur due to falls in elderly individuals with osteoporosis, or assaults involving sharp objects.
Pathophysiology
The pathophysiology of flail chest is complex, involving fractures of...
You might also read
Related Articles
Articles linked to this work by shared authors, journal, and citation graph.
Sort by
Same author
5-Fluorouracil With Microneedling Modulates Wound Healing in a Murine Model: An Immunohistochemical Analysis of Mechanism and Dose Efficacy.
Ophthalmic plastic and reconstructive surgery·2022
Same author
Isolated globe rupture without concomitant eyelid laceration or orbital trauma following facial dog bite injury in a child.
American journal of ophthalmology case reports·2022
Same author
Traumatic intrachoroidal nail implantation.
Proceedings (Baylor University. Medical Center)·2021